
Ankylosing spondylitis (pronounced ankle-oh-sing spon-dill-eye-tiss) is a form of arthritis that causes chronic (long-term) spine inflammation. Ankylosing spondylitis (AS) inflames the sacroiliac joints located between the base of the spine and pelvis. This inflammation, called sacroiliitis, is one of the first signs of AS. Inflammation often spreads to joints between the vertebrae, the bones that make up the spinal column. This condition is known as spondylitis. Some people with AS experience severe, persistent back and hip pain and stiffness. Others have milder symptoms that come and go. Over time, new bone formations may fuse vertebrae sections together, making the spine rigid. This condition is called ankylosis. How common is ankylosing spondylitis (AS)? Ankylosing spondylitis belongs to a group of diseases known as spondyloarthropathies. some three and 13 out of 1,000 Americans have one of these diseases. Who might have ankylosing spondylitis (AS)? Anyone can get AS, although it affects more men than women. Symptoms usually appear in people between the ages of 17 and 45. Ankylosing spondylitis has a genetic link and may run in families. SYMPTOMS AND CAUSES What causes ankylosing spondylitis (AS)? About 95% of people who have AS have a variation of the human leukocyte antigen-B gene (HLA-B). This changed, or mutated, gene produces a protein called HLA-B27 that increases disease risk. However, most people with a mutated HLA-B gene don’t get AS. In fact, 80% of children who inherit the mutated gene from a parent with AS don’t develop the disease. Some 60 genes have been linked to the condition. Having one of these conditions may also increase your risk: Crohn’s disease. Ulcerative colitis. Psoriasis. What are the symptoms of ankylosing spondylitis (AS)? Symptoms typically appear between the ages of 17 and 45 but may develop in younger children or older adults. Some people have persistent pain, while others experience milder symptoms. Symptoms may flare up (worsen) and improve (go into remission) off and on. If you have ankylosing spondylitis, you may experience: Lower back pain and stiffness. Hip pain. Joint pain. Neck pain. Difficulty breathing. Fatigue. Loss of appetite and unexplained weight loss. Abdominal pain and diarrhea . Skin rash. Vision problems. DIAGNOSIS AND TESTS How is ankylosing spondylitis (AS) diagnosed? There isn’t a test that definitively diagnoses ankylosing spondylitis. After reviewing your symptoms and family history, your healthcare provider will perform a physical exam. Your provider may order one or more of these tests to help guide diagnosis: Imaging scans: MRI( Magnetic Resonance Imaging) scans can detect spine problems earlier than traditional X-rays. Still, your provider may order spine x-rays to check for arthritis or rule out other problems. Blood tests: Blood tests can check for the presence of the HLA-B27 gene. About 8% of people of European descent have this gene, but only a quarter of them develop ankylosing spondylitis. MANAGEMENT AND TREATMENT What are the complications of ankylosing spondylitis (AS)? Ankylosing spondylitis may affect more than the spine. The disease may inflame joints in the pelvis, shoulders, hips and knees, and between the spine and ribs. People with AS are more prone to spinal fractures (broken vertebrae). Other complications include: Fused vertebrae (ankylosis). Kyphosis (forward curvature of the spine). Osteoporosis. Painful eye inflammation (iritis or uveitis) and sensitivity to light (photophobia). Heart disease, including aortitis, arrhythmia and cardiomyopathy. Chest pain that affects breathing. Jaw inflammation. Cauda equina syndrome (nerve scarring and inflammation). PREVENTION How can I prevent ankylosing spondylitis (AS)? Because ankylosing spondylitis has no known cause, there isn’t any way to prevent it. Stages of sarcoidosis Sarcoidosis can affect any part of the body, but it commonly impacts the lungs. Pulmonary sarcoidosis, or sarcoidosis of the lungs, can be categorized into four stages. Staging helps doctors understand how advanced the condition is. It can also help them understand which treatments might be right for you. A stage is assigned after a chest X-ray. This imaging test reveals several important factors about how the condition is affecting your lungs. Stage 1 to stage 4 are the crucial phases that progress from mild to advanced . OUTLOOK / PROGNOSIS What is the prognosis (outlook) for people who have ankylosing spondylitis (AS)? You should call your rheumatologist if you have AS and experience: Chest pain. Difficulty breathing. Vision problems. Severe back pain or other joint pain. Spine rigidity. Unexplained weight loss. The Takeaway : Ankylosing spondylitis symptoms may gradually worsen as you age. The condition is rarely disabling or life-threatening. Still, symptoms like joint pain may interfere with your ability to do the things you love. Early interventions can ease inflammation and pain. A combination of physical activity and prescribed medications from your rheumatologist can help.
Sjogren’s Syndrome: Symptoms, Causes, Diagnosis, Treatment
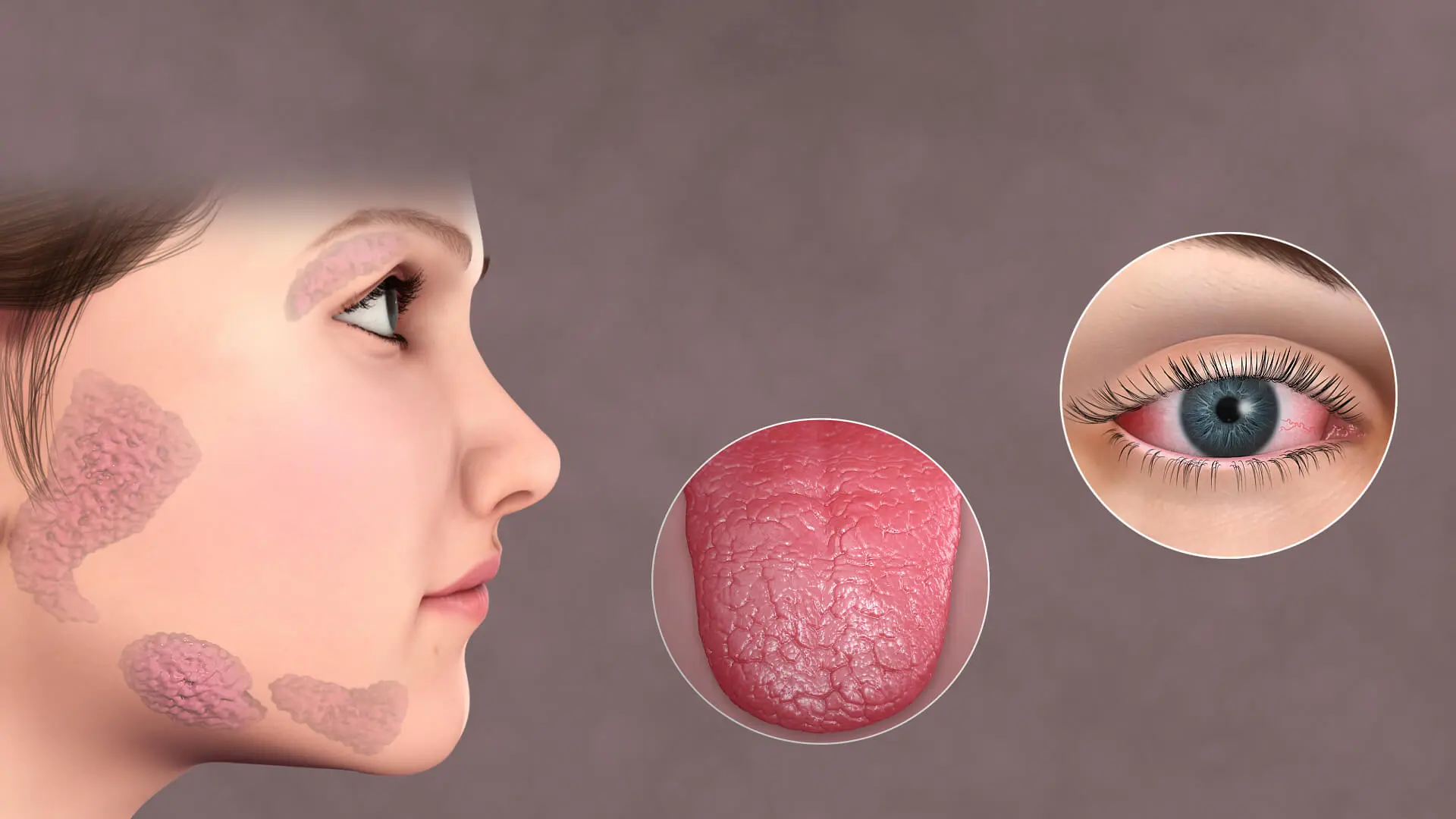
What Is Sjögren’s Syndrome? Sjögren’s (pronounced SHOW-grins) syndrome is a chronic autoimmune disorder in which the immune system attacks the body’s moisture-producing glands. It is most commonly identified by two hallmark symptoms: Dry eyes Dry mouth Sjögren’s syndrome often occurs alongside other autoimmune diseases such as Rheumatoid Arthritis and Lupus. The condition primarily affects the mucous membranes and glands responsible for producing tears and saliva, leading to reduced moisture levels in the eyes and mouth. Although it can develop at any age, it is most frequently diagnosed in individuals over 40 and is significantly more common in women. Sjögren’s Syndrome Symptoms Recognizing Sjögren’s syndrome symptoms early can help prevent complications. Main Symptoms Dry eyes (burning, itching, or gritty sensation) Dry mouth (difficulty swallowing or speaking, cotton-like feeling) Additional Symptoms Joint pain, swelling, and stiffness Swollen salivary glands (near the jaw and ears) Dry skin or skin rashes Vaginal dryness Persistent dry cough Prolonged fatigue What Causes Sjögren’s Syndrome? Sjögren’s syndrome is an autoimmune condition, meaning the immune system mistakenly attacks healthy tissues. While the exact cause remains unknown, several contributing factors include: Genetic predisposition Viral or bacterial infections (possible triggers) Immune system dysfunction The immune system primarily targets glands that produce tears and saliva but may also affect other organs such as: Joints Thyroid Kidneys Liver Lungs Skin Nerves Risk Factors for Sjögren’s Syndrome Certain factors increase the likelihood of developing the condition: Age (most common after 40) Gender (more prevalent in women) Existing autoimmune or rheumatic diseases Sjögren’s Syndrome Diagnosis Diagnosis often involves a combination of symptom evaluation and medical testing. A specialist (rheumatologist) may ask questions such as: Do your symptoms worsen throughout the day or outdoors? Do you have existing conditions like arthritis or high blood pressure? Have you recently started new medications? Do autoimmune diseases run in your family? Additional tests may include: Eye tests to measure tear production Saliva flow tests Blood tests for autoimmune markers Sjögren’s Syndrome Complications If not managed properly, Sjögren’s syndrome can lead to several complications: Oral Health Issues Increased risk of dental cavities Oral thrush (yeast infections) Eye Complications Light sensitivity Blurred vision Corneal damage Systemic Complications Lung, kidney, or nerve involvement Chronic fatigue impacting daily life Sjögren’s Syndrome Treatment Options There is no cure for Sjögren’s syndrome, but treatment focuses on relieving symptoms and preventing complications. 1. Artificial Tears & Hydration Over-the-counter eye drops for dry eyes Frequent water intake for dry mouth 2. Prescription Medications Drugs to stimulate saliva production Anti-inflammatory medications for systemic symptoms 3. Surgical Option (Punctual Occlusion) A minor procedure that blocks tear ducts to retain moisture in the eyes. Silicone or collagen plugs are inserted to help preserve natural tears. Living With Sjögren’s Syndrome Managing Sjögren’s syndrome requires a proactive approach: Stay hydrated throughout the day Maintain good oral hygiene Use lubricating eye drops regularly Work closely with a rheumatologist Monitor for symptoms affecting other organs Summary Sjögren’s syndrome is a chronic autoimmune disease that primarily causes dry eyes and dry mouth but can also affect multiple organs. Early diagnosis and proper management can significantly improve quality of life and reduce complications. ⚠️ Medical Disclaimer This content is for informational purposes only and should not be considered medical advice. Always consult a qualified healthcare provider or rheumatologist for diagnosis and treatment tailored to your condition.

Scleroderma: Definition, Types, Symptoms, Causes
Systemic scleroderma is an autoimmune rheumatic disease characterized by excessive production and accumulation of collagen, called fibrosis, in the skin and internal organs, and by injuries to small arteries. There are two major subgroups of systemic sclerosis based on the extent of skin involvement. Limited and diffuse. The limited form affects areas below, but not above the elbows and knees with or without involvement of the face. The diffuse form also affects the skin above the elbows and knees and can also spread to the torso. Also… Kidneys, heart, lungs, and gastrointestinal tract can also be affected by the fibrotic process. Patients with limited systemic sclerosis have a better prognosis than those with the diffuse form. Death is most often as a result of lung, heart, and kidney. Skin symptoms In the skin, systemic sclerosis causes hardening and scarring. The skin may appear tight, reddish, or scaly. The severity of these symptoms varies greatly among patients. Some having scleroderma of only a limited area of the skin (such as the fingers) and little involvement of the underlying tissue, while others have progressive skin involvement. Open wounds especially on fingertips (digital ulcers) and sometimes on the knuckles, are not uncommon. Diffuse scleroderma can cause musculoskeletal, pulmonary, gastrointestinal, renal, and other complications. Over 80 percent of most patients have vascular symptoms and Raynaud’s phenomenon, which leads to attacks of discoloration of the hands and feet in response to the cold. Calcinosis is the deposition of calcium in lumps under the skin is also common in systemic scleroderma, and is often spotted near the elbows, knees, or other joints. Lung impairment is universally seen with diffuse scleroderma patients. Diffuse scleroderma can affect and decrease motility in any part of the gastrointestinal tract. Scleroderma is also associated with watermelon stomach. This is a condition in which atypical blood vessels proliferate in a radial pattern around the stomach. Cause No clear cause for scleroderma and systemic sclerosis has been identified, genetic predisposition appears to be limited, still , a familial predisposition for autoimmune disease is common . Diagnosis Diagnosis is usually by clinical suspicion, presence of auto antibodies, and occasionally by biopsy. Diagnostic hints that another disorder is responsible include the absence of Raynaud’s phenomenon , a lack of abnormalities in the skin on the hands , a lack of internal organs involvement , a normal nuclear antibodies test result . Treatment No cure for scleroderma is known, but treatment exists for some of the symptoms, including drugs that soften the skin and reduce inflammation. Some patients may benefit from exposure to heat as well. Consultation with a seasoned rheumatologist is useful in view of the complex nature of the disease symptoms and progress. Topical \ symptomatic Topical treatment for the skin changes of scleroderma do not alter the disease course, but may improve pain and ulceration. A range of nonsteroidal anti inflammatory drugs (NSAIDS), such as naproxen, can be used to ease painful symptoms. The benefits of steroids such as prednisolone is limited. Skin tightness may be treated systematically with methotrexate, while skin thickness can be treated with penicillamine. The Takeaway Treatments for SS have drastically improved in the past three decades. Although there’s still no cure for SS, there are many different treatments that can help you manage your symptoms. It may be a good idea to talk with your rheumatologist if any of your symptoms are getting in the way of your daily life. They can work with you to adjust your treatment plan to help you cope with this chronic condition.

Sarcoidosis: Causes, Symptoms & Treatment
Sarcoidosis is an inflammatory disease in which granulomas, or clumps of inflammatory cells, form in various organs. This causes organ inflammation. Sarcoidosis may be triggered by your body’s immune system responding to foreign substances, such as viruses, bacteria, or chemicals. The areas of the body commonly affected by sarcoidosis include: lymph nodes | lungs |eyes | skin | liver | heart | spleen |brain What are the symptoms of sarcoidosis? Some people with sarcoidosis don’t have any symptoms. However, general symptoms may include: fatigue fever weight loss joint pain dry mouth nosebleeds Symptoms vary depending on the part of your body that’s affected by the disease. Sarcoidosis can occur in any organ, but it most commonly affects the lungs. Lung symptoms can include: a dry cough shortness of breath wheezing chest pain around your breastbone Skin symptoms can include: skin rashes skin sores hair loss What causes sarcoidosis? The exact cause of sarcoidosis is unknown. However, sex, race, and genetics can increase the risk of developing the condition: Sarcoidosis is more common in women than in men. People of African American descent are three times more likely to develop the condition than white people. They’re also more likely to have severe disease. People with a family history of sarcoidosis have a significantly higher risk of getting the disease. Sarcoidosis rarely occurs in children. Symptoms usually appear in people between the ages of 20 and 40. How is sarcoidosis diagnosed? It can be difficult to diagnose sarcoidosis. Symptoms can be similar to those of other diseases, such as arthritis or cancer. Your doctor will run a variety of tests to make a diagnosis. Your rheumatologist will first perform a physical examination to: check for skin bumps or a rash look for swollen lymph nodes listen to your heart and lungs check for an enlarged liver or spleen Based on the findings, your doctor may order additional diagnostic tests and blood tests to check your kidney and liver function. Stages of sarcoidosis Sarcoidosis can affect any part of the body, but it commonly impacts the lungs. Pulmonary sarcoidosis, or sarcoidosis of the lungs, can be categorized into four stages. Staging helps doctors understand how advanced the condition is. It can also help them understand which treatments might be right for you. A stage is assigned after a chest X-ray. This imaging test reveals several important factors about how the condition is affecting your lungs. Stage 1 to stage 4 are the crucial phases that progress from mild to advanced . How is sarcoidosis treated? There’s no cure for sarcoidosis. However, some people do not need treatment for sarcoidosis. Symptoms often improve without treatment. This is called “spontaneous remission.” Treatment may be needed if the disease affects your: eyes lungs heart nervous system If you do need treatment, your doctor will assess your symptoms and how advanced the condition is. They may prescribe medications to help suppress the immune system and reduce inflammation. This can ease the symptoms of sarcoidosis. Medications used to treat sarcoidosis include: Corticosteroids. Prednisone is the most commonly prescribed treatment for sarcoidosis. However, the side effects of this medication can be severe, so it may only be prescribed for a short period of time. Disease modifying antirheumatic drugs (DMARDs). DMARDs are medications that suppress the immune system. They may slow the progression of sarcoidosis and reduce symptoms. Examples include methotrexate (Trexall), azathioprine (Azasan), and leflunomide (Arava). Antimalarial agents. Medications like hydroxychloroquine (Plaquenil) may be helpful for sarcoidosis symptoms that affect the skin and joints. Biologic agents. These medications are used to stop an overactive immune system. They have significant side effects, so they’re typically reserved for people whose bodies do not tolerate other medications. Examples include rituximab (Rituxan), infliximab (Remicade), and golimumab (Simponi). The length of any treatment will vary. Some people take medication for 1 to 2 years. Other people may need to take medication for much longer. What are the potential complications of sarcoidosis? Most people who receive a diagnosis of sarcoidosis don’t experience complications. However, sarcoidosis can become a chronic, or long-term, condition. Other potential complications may include: lung infection retinal damage from chronic inflammation cataracts , which are characterized by clouding of the lens in your eye In rare cases, sarcoidosis causes severe heart and lung damage. If this occurs, you may need immunosuppressive medications. It’s important to contact your doctor if you have: breathing difficulties heart palpitations , which occur when your heart is beating too fast or too slow changes in your vision or loss of vision eye pain sensitivity to light facial numbness These can be signs of dangerous complications. Your doctor may recommend that you see an optometrist or ophthalmologist because this disease can affect your eyes without causing immediate symptoms. What is the outlook for someone with sarcoidosis? The outlook is generally good for people with sarcoidosis. Many people live relatively healthy, active lives. Symptoms often improve with or without treatment in about 2 years. In some cases, however, sarcoidosis can become a long-term condition. If you need help coping, you can talk with a rheumatologist or join a sarcoidosis support group.

Everything You Want to Know About Rheumatoid Arthritis
Rheumatoid Arthritis: Understanding Symptoms, Causes, and Treatment Rheumatoid arthritis (RA) is an autoimmune disease that causes joint pain, inflammation, and progressive damage throughout the body. One of the defining characteristics of RA is that it typically affects joints symmetrically. This means if a joint in one arm or leg is affected, the same joint on the opposite side is likely to be affected as well. This pattern helps doctors distinguish RA from other types of arthritis. RA is a chronic condition marked by periods of increased symptoms—known as flares or exacerbations—and periods of remission, during which symptoms may reduce significantly or disappear altogether. While RA commonly affects joints in the hands, wrists, and knees, it can also impact other parts of the body, including the lungs, heart, and eyes. Rheumatoid Arthritis Symptoms RA can be difficult to diagnose because symptoms vary from person to person and may come and go. Common signs doctors look for include: Joint pain, swelling, and stiffness (especially in small joints like hands, wrists, and feet) Symptoms lasting more than 6 weeks Morning stiffness lasting at least 30 minutes Pain in multiple joints Tenderness and swelling in more than one joint Low-grade fever Symmetrical joint involvement (both sides of the body) Fatigue Loss of appetite Causes and Risk Factors RA is an autoimmune disorder, meaning the immune system mistakenly attacks healthy body tissues. While the exact cause is still unknown, several factors may increase the risk: Age Gender (more common in women) Genetics Smoking Obesity Diet If left untreated, RA can lead to joint damage, loss of alignment, and eventual joint destruction. Diagnosis of Rheumatoid Arthritis To diagnose RA, healthcare providers may use a combination of physical examinations, blood tests, and imaging such as X-rays. Patients are often referred to a specialist known as a rheumatologist, who may assess: Reflexes and muscle strength Joint swelling and redness Range of motion and joint function Warmth and tenderness in affected joints These tests help determine not only the presence of RA but also the severity of joint damage. Possible Complications If not properly managed, RA can lead to serious complications, including: Joint damage and deformity Increased risk of heart disease Carpal tunnel syndrome Lung conditions such as pneumonia and pulmonary fibrosis Chest pain Rheumatoid Arthritis Treatment A diagnosis of RA can feel overwhelming, but effective treatments are available to manage symptoms and slow disease progression. 1. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) These medications help reduce pain and inflammation but do not slow disease progression. Common over-the-counter options include ibuprofen and naproxen. 2. DMARDs (Disease-Modifying Anti-Rheumatic Drugs) DMARDs work by suppressing the immune system to slow or stop the progression of RA. These are prescription medications such as methotrexate (Trexall). 3. Biologics When traditional DMARDs are not effective, biologics may be prescribed. These target specific parts of the immune system involved in inflammation. Examples include etanercept (Enbrel) and tocilizumab. 4. Steroids Steroids are often used during severe flares to reduce inflammation and pain. They may be prescribed short-term or, in some cases, for longer durations. Common examples include: Hydrocortisone (Cortef) Methylprednisolone (Medrol) Prednisone (Deltasone) While steroids can help control symptoms and prevent further damage, they do not reverse existing joint damage. Rheumatoid Arthritis Diet Diet can play a supportive role in managing RA symptoms. Recommended foods include: High-fiber foods such as broccoli and berries Antioxidant-rich foods like spinach, kidney beans, and pecans Omega-3 fatty acids found in salmon, tuna, and herring Summary Rheumatoid arthritis can cause significant pain and, if left untreated, may lead to joint deformities—especially in the hands and feet. These deformities can result in a curved, claw-like appearance of the fingers and toes. However, early diagnosis and proper treatment can significantly reduce the risk of severe complications. Working closely with a rheumatologist to develop an effective treatment plan is key to managing RA and maintaining quality of life. Medical Disclaimer This content is for informational purposes only and should not be considered medical advice. Always consult a qualified healthcare professional or rheumatologist for diagnosis and treatment tailored to your condition.

Reactive arthritis | Causes, symptoms, treatments
What Is Reactive Arthritis? Reactive arthritis is a type of inflammatory arthritis that affects the joints, eyes, urinary tract (urethra), and skin. It is often referred to as a post-infectious arthritis, meaning it develops in response to an infection elsewhere in the body. The condition may develop gradually with periods of remission and recurrence, or it may appear suddenly with severe symptoms. Reactive arthritis most commonly affects sexually active men between the ages of 20 and 40, and individuals living with HIV may have a higher risk. What Causes Reactive Arthritis? The exact cause of reactive arthritis is not fully understood. However, research suggests a strong link to genetic and infectious factors. Key Causes and Triggers: Genetic predisposition, particularly the HLA-B27 marker Sexually transmitted infections such as Chlamydia trachomatis Gastrointestinal infections (from contaminated food or water) Reactive arthritis typically develops after an infection, even when the infection itself has already resolved. While practicing safe sex (e.g., condom use) can reduce the risk of certain infections, there is no guaranteed way to prevent reactive arthritis. Reactive Arthritis Symptoms Symptoms often appear 1 to 4 weeks after an infection and may affect different parts of the body. Early Symptoms Painful urination Discharge from the penis (in men) Diarrhea (if intestinal infection is involved) Joint Symptoms Pain and swelling in joints (knees, ankles, feet, hips) Inflammation in fingers and toes Usually affects one or a few joints at a time Additional Symptoms Mouth ulcers Eye inflammation (redness, pain, blurred vision) Enthesitis (pain where tendons and ligaments attach to bone) Scaly skin rashes (especially on palms, soles, or scalp) Lower back pain due to sacroiliac joint involvement How Is Reactive Arthritis Diagnosed? Diagnosing reactive arthritis can be challenging because symptoms may not appear all at once. There is no single test for the condition, but a rheumatologist may use: Medical history and symptom review Testing urethral discharge for sexually transmitted infections Stool tests to detect gastrointestinal infections Blood tests (including genetic markers like HLA-B27) Joint examination for inflammation Reactive Arthritis Treatment Treatment focuses on managing symptoms and addressing the underlying infection. 1. NSAIDs (Pain and Inflammation Relief) Nonsteroidal anti-inflammatory drugs such as ibuprofen and naproxen are commonly used to reduce pain and swelling. 2. Antibiotics If a bacterial infection (such as Chlamydia trachomatis) is identified, antibiotics are prescribed to treat the infection. 3. Steroids Steroids may be used to treat: Joint inflammation Skin conditions Eye inflammation 4. Physical Therapy & Exercise Patients with persistent symptoms may benefit from guided exercise programs to maintain joint mobility and strength. Complications of Reactive Arthritis Although many people recover fully, some may experience complications, including: Chronic arthritis Recurring symptoms Inflammation of the heart muscle Eye complications such as glaucoma Prognosis: What to Expect The outlook for reactive arthritis varies from person to person. Most people recover within 3 to 4 months About 50% may experience recurrence over time A small number may develop long-term or chronic symptoms Early diagnosis and treatment significantly improve outcomes. Living With Reactive Arthritis Managing reactive arthritis involves: Seeking early medical care after infections Practicing safe sex to reduce STI risk Following prescribed treatment plans Staying physically active to support joint health Regular follow-ups with a rheumatologist Summary Reactive arthritis is an inflammatory condition triggered by infections, affecting joints and other parts of the body. While it can be uncomfortable and sometimes recurrent, most people recover fully with proper treatment and care. ⚠️ Medical Disclaimer This content is for informational purposes only and does not substitute professional medical advice. Always consult a qualified healthcare provider or rheumatologist for proper diagnosis and treatment.

Raynaud’s Disease & Syndrome: Symptoms, Causes, Treatment
What Is Raynaud’s Phenomenon? Do your fingers or toes suddenly become cold, pale, and numb when exposed to cold temperatures? You may be experiencing Raynaud’s phenomenon, a condition that causes temporary “attacks” where blood flow to certain areas—usually the fingers and toes—is reduced. During an attack: Affected areas may turn white or blue They feel cold and numb As blood flow returns, they may tingle, throb, or hurt In most cases, Raynaud’s is not serious. While there is no cure, symptoms can be effectively managed through lifestyle adjustments and medical treatment when necessary. What Causes Raynaud’s Phenomenon? The exact cause of Raynaud’s is not fully understood. However, it is known to occur when blood vessels overreact and spasm in response to: Cold temperatures Emotional stress Anxiety These spasms temporarily restrict blood flow to the affected areas. Types of Raynaud’s Phenomenon Primary Raynaud’s (Raynaud’s Disease) This is the most common and less severe form. Occurs without an underlying medical condition Typically develops between ages 15 and 30 Symptoms are usually mild May improve over time without treatment Primary Raynaud’s is not linked to other diseases, and most people do not develop complications. Secondary Raynaud’s (Raynaud’s Syndrome) This form is more serious and occurs due to an underlying condition. It is often associated with autoimmune diseases such as Scleroderma. Possible Causes: Diseases affecting blood vessels or connective tissue Medications that narrow blood vessels or affect blood pressure Nerve damage in hands or feet Repetitive motion injuries (e.g., use of vibrating tools like jackhammers) Secondary Raynaud’s typically develops after age 40 and may lead to more severe complications. Raynaud’s Symptoms A Raynaud’s “attack” can affect: Fingers and toes (most common) Nose Ears Lips Nipples Common Symptoms: Cold, numb, or painful fingers and toes Skin turning white, pale, or bluish Tingling, throbbing, or burning when blood flow returns Swelling after an attack Attacks can last from a few seconds to several hours and may begin in one finger or toe before spreading. Who Is at Risk? Women (more commonly affected) People living in colder climates Individuals over 30 (for secondary Raynaud’s) Workers exposed to repetitive vibration (e.g., machinery operators) How Is Raynaud’s Phenomenon Diagnosed? A rheumatologist will typically: Review your medical history and symptoms Examine your hands and feet Conduct cold stimulation tests (e.g., placing hands in cold water) Use microscopy to examine small blood vessels Order blood tests to distinguish between primary and secondary Raynaud’s Raynaud’s Treatment Options Treatment depends on the severity and type of Raynaud’s. Lifestyle & Home Management Managing triggers is the first line of defense: Dress warmly (gloves, socks, hats) Warm your car before driving in cold weather Avoid sudden exposure to cold (e.g., use gloves when handling frozen items) Use hand and foot warmers Manage stress through relaxation techniques During an Attack: Rub hands and feet Wiggle fingers and toes Place hands under warm areas (like underarms) Practice deep breathing to reduce stress Medications If symptoms interfere with daily life, your doctor may prescribe: Calcium channel blockers ACE inhibitors Alpha blockers Prescription topical creams These medications help improve blood flow and reduce the frequency of attacks. Surgical Options (Rare Cases) In severe cases, procedures such as nerve-blocking injections or surgery may be considered to improve blood circulation and prevent tissue damage. Complications of Raynaud’s Phenomenon Most cases are mild, but severe secondary Raynaud’s can lead to: Skin sores or ulcers Tissue damage Increased risk of infection Summary Raynaud’s phenomenon is a condition that affects blood flow to extremities, causing cold, numb, and discolored fingers or toes. While it can be uncomfortable, most cases are manageable with lifestyle changes and proper care. Early diagnosis is important, especially for identifying secondary Raynaud’s linked to underlying conditions. ⚠️ Medical Disclaimer This content is for informational purposes only and does not substitute professional medical advice. Always consult a qualified healthcare provider or rheumatologist for proper diagnosis and treatment.

Psoriatic arthritis | Causes, symptoms, treatments
What Is Psoriatic Arthritis? Psoriatic arthritis (PsA) is a chronic inflammatory autoimmune disease that affects both the skin and joints. It is closely linked to Psoriasis, a skin condition that causes red, scaly patches—commonly on the elbows, knees, scalp, and hands. In PsA, the immune system mistakenly attacks healthy tissues, leading to joint pain, swelling, and stiffness. If left untreated, the inflammation can cause long-term joint damage and reduced mobility. Psoriatic Arthritis Symptoms Recognizing psoriatic arthritis symptoms early is key to preventing complications. Common Symptoms: Morning stiffness and fatigue Swollen fingers and toes (dactylitis) Joint pain and stiffness Scaly skin patches (especially on elbows, knees, and scalp) Pain and swelling around tendons (enthesitis) Foot pain (especially in the heel) Eye redness and pain Lower back pain Reduced range of motion Nail changes (pitting, discoloration) PsA may sometimes resemble Rheumatoid Arthritis, but unlike RA, it does not always affect joints symmetrically. Types of Psoriatic Arthritis Psoriatic arthritis varies in severity and presentation. Oligoarticular PsA A milder form Affects four or fewer joints Polyarticular PsA More severe Affects four or more joints Can resemble rheumatoid arthritis What Causes Psoriatic Arthritis? The exact cause is unknown, but several factors contribute: Immune system dysfunction Genetic predisposition (family history) Infections (e.g., strep throat triggering psoriasis) Environmental triggers Psoriatic Arthritis Risk Factors Having psoriasis (about 30% develop PsA) Age (commonly between 30–50, but can occur at any age) Family history of autoimmune or joint diseases Equal prevalence in men and women How Is Psoriatic Arthritis Diagnosed? There is no single test for PsA. Diagnosis typically involves: Imaging tests (X-rays, MRI scans) Blood tests to detect inflammation Joint fluid analysis Skin examination or biopsy A rheumatologist will evaluate symptoms and rule out other forms of arthritis. Psoriatic Arthritis Treatment Options While there is no cure, psoriatic arthritis treatment focuses on controlling inflammation, relieving symptoms, and preventing joint damage. Medications NSAIDs (e.g., ibuprofen) for pain relief DMARDs to slow disease progression Biologics to target inflammation-causing proteins Enzyme inhibitors to reduce inflammatory processes Steroids (used cautiously due to side effects) Surgical Treatment In severe cases, joint replacement surgery may be considered. Lifestyle Changes for Psoriatic Arthritis Lifestyle adjustments play a major role in managing PsA: Engage in low-impact exercises (walking, swimming) Maintain a healthy weight Avoid smoking Limit alcohol intake Consider supportive therapies like massage or acupuncture Psoriatic Arthritis Flare Triggers Understanding triggers can help reduce flare-ups: Stress Infections Weight gain Skin injuries (cuts, scrapes, sunburn) Psoriatic Arthritis Complications If not properly managed, PsA can lead to: Chronic fatigue Depression and anxiety Fibromyalgia Gout Permanent joint damage Outlook: Living With Psoriatic Arthritis There is currently no cure for psoriatic arthritis, but with early diagnosis and proper treatment, many people achieve remission or significant symptom control. Working closely with a rheumatologist ensures a personalized treatment plan and better long-term outcomes. Summary Psoriatic arthritis is an autoimmune condition that affects both the skin and joints, often developing in people with psoriasis. Early intervention, proper treatment, and lifestyle changes can help manage symptoms, prevent complications, and improve quality of life. ⚠️ Medical Disclaimer This content is for informational purposes only and does not substitute professional medical advice. Always consult a qualified healthcare provider or rheumatologist for proper diagnosis and treatment.

Polymyositis: Symptoms, Causes, Diagnosis, Treatment
What Is Polymyositis? Polymyositis is a rare inflammatory muscle disease that causes progressive muscle weakness, particularly in muscles closest to the center of the body (such as the hips, thighs, shoulders, and upper arms). It is considered an autoimmune condition, meaning the immune system mistakenly attacks healthy muscle tissue, leading to inflammation and muscle damage. The disease typically develops gradually over time and rarely affects individuals under the age of 18. It is more common in women than men, with a ratio of approximately 2:1. Polymyositis Symptoms Recognizing polymyositis symptoms early is key to managing the disease effectively. Common Symptoms: Muscle weakness (especially near the trunk of the body) Difficulty rising from a seated position Trouble climbing stairs or lifting objects Difficulty getting up after lying down Difficulty swallowing (dysphagia) Muscle aches and tenderness Fatigue and low-grade fever Shortness of breath (due to lung or heart involvement) Weight loss Some individuals may also experience: Skin changes such as a reddish or violet rash around the eyes Raynaud’s Phenomenon (cold, discolored fingers or toes due to reduced blood flow) What Causes Polymyositis? The exact cause of polymyositis is unknown, but it is strongly linked to immune system dysfunction. Possible contributing factors include: Autoimmune response targeting muscle tissue Genetic predisposition Environmental triggers Polymyositis may also be associated with other autoimmune diseases. How Is Polymyositis Diagnosed? Diagnosing polymyositis involves a combination of clinical evaluation and specialized tests. Common Diagnostic Methods: Blood tests: Elevated muscle enzymes indicate muscle damage Urine tests: Check for organ involvement Muscle biopsy: Confirms inflammation in muscle tissue Electromyography (EMG): Detects abnormal muscle electrical activity Early diagnosis is essential to prevent complications and improve outcomes. Polymyositis Treatment Options While there is no cure, polymyositis treatment focuses on reducing inflammation, improving muscle strength, and preventing complications. 1. Corticosteroids High-dose corticosteroids are usually the first line of treatment to reduce muscle inflammation. 2. Immunoglobulin Therapy (IVIG) Intravenous immunoglobulin (IVIG) may be used in severe cases to improve muscle strength and immune function. 3. Physical Therapy A structured rehabilitation program helps restore muscle strength, mobility, and function. Complications of Polymyositis If not properly managed, polymyositis can lead to serious complications: Difficulty swallowing (leading to malnutrition and weight loss) Aspiration pneumonia (due to food or liquid entering the lungs) Breathing problems (if chest muscles are affected) Risk of respiratory failure in severe cases Outlook: Living With Polymyositis The prognosis for polymyositis varies depending on severity and response to treatment. Many patients respond well to early treatment Muscle strength can improve significantly with therapy Some degree of weakness may persist Symptoms may recur (flare-ups) over time Although polymyositis is rarely life-threatening, untreated cases can lead to long-term disability. Summary Polymyositis is a rare autoimmune muscle disease that causes progressive weakness and inflammation. Early diagnosis and treatment are essential to manage symptoms, prevent complications, and improve quality of life. Working closely with a rheumatologist ensures a tailored treatment plan and better long-term outcomes. ⚠️ Medical Disclaimer This content is for informational purposes only and does not substitute professional medical advice. Always consult a qualified healthcare provider or rheumatologist for proper diagnosis and treatment.

Osteoporosis: Symptoms, Causes, Tests & Treatment
Osteoporosis: What You Need to Know Osteoporosis weakens bones, making them more susceptible to sudden and unexpected fractures. It means you have reduced bone mass and strength. The disease often progresses without symptoms or pain and is usually not discovered until weakened bones lead to fractures—most commonly in the hip, wrist, and spine. What Causes Osteoporosis? Your bones are made of living, growing tissue. The inside of healthy bones looks like a sponge. When osteoporosis occurs, the “holes” in that sponge grow larger and more numerous, weakening the bone. Bone remodeling helps supply the body with needed calcium while keeping bones strong. However, after age 35, bone breakdown begins to occur faster than bone buildup, leading to a gradual loss of bone mass. If you are experiencing menopause or already have osteoporosis, this breakdown happens even more rapidly. Osteoporosis Symptoms Osteoporosis is often called a “silent disease” because there are usually no visible symptoms. However, you should watch out for the following signs: Bone fractures Changes in posture (stooping or bending forward) Shortness of breath (due to reduced lung capacity from compressed discs) Loss of height (getting shorter by an inch or more) Lower back pain Who Is at Risk? Your risk of developing osteoporosis depends on several factors, including age, gender, and lifestyle: Risk increases with age (women over 50 are at the highest risk) Ethnicity plays a role (Caucasian and Asian women are more likely to develop osteoporosis, but African American and Hispanic women are also at risk) Family history can increase your chances Diets low in calcium and vitamin D contribute to bone loss Lifestyle habits like smoking and excessive alcohol use can increase risk Osteoporosis Diagnosis Your healthcare provider can assess your bone health before problems begin. A Bone Mineral Density (BMD) test is commonly used for diagnosis. Women over the age of 65 should have a BMD test Men over the age of 70 should also consider screening Treatment for Osteoporosis Treatment may include a combination of exercise, supplements, and medication. Consider incorporating: Weight-bearing exercises Resistance training Balance exercises Supplementation with calcium and vitamin D is often recommended to help prevent or manage osteoporosis. Osteoporosis Medications There is no single “best” medication for osteoporosis—the right treatment depends on your individual condition. Common options include: Bisphosphonates (help prevent bone loss by slowing bone resorption) Biologics, such as Denosumab Calcium Intake Guidelines The recommended daily calcium intake is 1,000 mg to 1,200 mg, obtained through diet and/or supplements. Taking more than this amount may increase the risk of: Kidney stones Calcium buildup in blood vessels Constipation Always consult your healthcare provider before starting supplements. Living with Osteoporosis Managing osteoporosis involves making lifestyle adjustments: Get regular exercise Avoid excessive caffeine and alcohol Eat a balanced, nutrient-rich diet Reduce fall risks at home (use grab bars and stair railings) Summary You can still lead an active and fulfilling life with osteoporosis. Always consult your rheumatologist if: You experience a fall You develop sudden or severe back pain Working closely with a healthcare professional will help you manage the condition effectively and maintain your quality of life.